Medical Devices Safety Update, Volume 2, Number 3, May 2014
Medical Devices Safety Update is the medical device safety bulletin of the Therapeutic Goods Administration (TGA)
In this issue
Alarm hazards - user error a common contributing factor
Alarm hazards continue to contribute to significant mortality and morbidity issues in Australian healthcare settings, with user error listed as one of the most common contributing factors.
In the 38 months between 1 January 2011 and 28 March 2014, the TGA's medical device Incident and Reporting Investigation Scheme (IRIS) database recorded a total of 343 reports which listed an alarm issue as a factor in an incident. Of these reports, 19 related to incidents in which a patient died. User error was listed as a factor in 10 of these cases, one case involved a battery issue and in eight cases investigators found no fault with the device. See Table 1 for more details.
During its investigations, the TGA has found that many incidents associated with alarm systems failure are attributed to user error, but often the root causes can be inherent design deficiencies.
| Table 1: Causes of fatal incidents associated with alarm systems failure and user error | |
|---|---|
| Cause | Number |
| Volume turned down | 2 |
| Alarm silenced | 4 |
| Alarm ignored | 2 |
| User did not follow Instructions for Use | 2 |
| Total | 10 |
| Type of device involved | Number |
| Monitor | 6 |
| Ventilator | 1 |
| Syringe pump | 1 |
| Blood warmer | 1 |
| Insulin pump | 1 |
| Total | 10 |
The TGA's investigations have found that poorly designed devices can often enable and induce user errors, and worsen the consequences associated with user errors.
Eleven recalls were required due to design issues.
As reported in Medical Devices Safety Update's January edition, the Emergency Care Research Institute (ECRI) has ranked alarm issues as the number one health technology hazard for 2014, after giving them the same ranking in 2012 and 2013.1 The ECRI is an international, independent, non-profit organisation that researches the best approaches to improving patient care.
The TGA has been represented on the international committee responsible for overseeing the development of technical standards covering the safety and effectiveness of medical electrical equipment.
The alarm systems collateral standard tries to differentiate the responsibilities between the responsible organisation (the hospital/healthcare facility, or the head of the department responsible) and the individual user. This international standards committee has considered extensive evidence that one of the biggest reasons contributing to user error is alarm fatigue.
When health professionals become exhausted by alarm fatigue they tend to ignore them, develop unsafe ways to prioritise or adjust alarm limits, and became less likely to respond to any alarm.
Since user error can never be totally prevented, the Essential Principles contained within Australia's medical device regulations place a responsibility on manufacturers to mitigate risks.
Manufacturers must select appropriate solutions for the design and construction of medical devices to minimise any risks associated with their use, including foreseeable misuse.
The Essential Principles also require that the measurement, monitoring and display scale of devices must be designed and produced in accordance with ergonomic principles, having regard to the intended purpose of the device.
While manufacturers are responsible for selecting appropriate design and construction solutions to ensure the quality and safety of their devices in relation to their intended use, the healthcare facilities using these devices also have obligations to ensure effective alarm management programs are in place.
It is important that the responsible organisations configure their alarm systems so that operators are not able to compromise them.
Alarm failures are 'systems' issues that cannot be solved by any single stakeholder group alone.
In working towards effective solutions the TGA believes the following tips can be helpful to reduce alarm-related adverse events:
- health facilities should:
- set up effective alarm management programs that involve clinicians, biomedical engineers, hospital management and administrative staff.
- ensure that responsibilities are clearly assigned to the relevant personnel.
- ensure all staff carefully read and fully understand the Instructions for Use.
- manufacturers should:
- apply usability and ergonomic principles in the design and construction of their devices to assure their devices comply with quality and safety requirements.
- ensure that the Instructions for Use be clearly written and that user education is appropriately designed and effectively conducted.
- both health facilities and manufacturers have the responsibility to establish effective communication systems to reduce adverse events. With effective communication and proper user training, users can become familiar with alarm functionalities and can confidently and competently apply these functions to meet their purposes.
The TGA relies on the public, health professionals and industry to report problems with medicines, vaccines and medical devices - this allows us to identify and respond to safety matters.
For further information about reporting adverse events, visit the 'Report a problem' webpage on the TGA website.
Identifying options for immediate action
Regulators and other stakeholders around the world have been discussing ways to tackle alarm issues in healthcare settings for some time.
Here are 10 actions that health facilities can take immediately to improve alarm conditions and reduce alarm fatigue:
- Gain cross-disciplinary leadership support to show a compelling need for action.
- Establish a cross-functional team with clinical leadership to address alarm fatigue across all environments of care.
- Re-establish priorities: process should drive technology adoption rather than allowing technology to drive the process.
- Develop a continuous improvement process for constantly optimising alarm system policies and configurations. Example: Improvement strategy based on crawl-walk-run.
- Conduct clinical testing and analyse alarm data to implement optimised alarm limits and delays (both alarm condition and alarm signal generation delays) and to reduce clinically non-actionable alarm conditions.
- Test acoustics on clinical floors: environmental noise impacts patient and staff well-being and patient safety.
- Implement an alarm system configuration policy based on clinical evidence.
- Change single-use sensors more frequently to reduce nuisance alarm conditions (except in paediatric units).
- Mandate alarm system management training for all clinical operators.
- Share experiences with regulators and other bodies with problem reporting systems so everyone can benefit from your efforts in a cross-disciplinary way.
Reference
- Top 10 Health technology Hazards for 2014, Health Devices, volume 42, issue 11, November 2013. Emergency Care Research Institute.
Further information
Further alarm safety resources can be found on the ECRI website.
Adjustments to plunger forces for new BD 50 ml Plastipak syringes
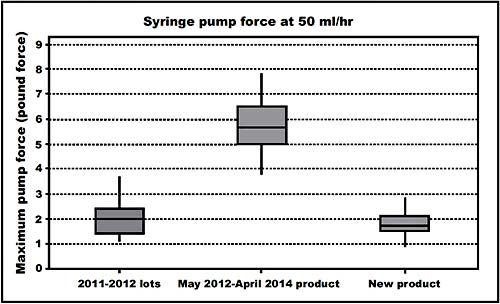
Healthcare facilities and biomedical engineers are advised that new stock of Becton Dickinson BD 50 ml Plastipak syringes has lower plunger resistance forces compared to the stock that has been available for the past two years. Health professionals are advised that adjustments may be needed to syringe drivers used with BD Plastipak 50 ml syringes to ensure their occlusion alarm settings reflect the change.
BD Plastipak 50 ml syringes with BD catalogue number 300865 supplied after 14 April 2014 and those syringes with BD catalogue number 300869 to be supplied from June/July 2014 will have similar plunger forces to products that were available before May 2012.
For the period May 2012 to April 2014, BD Plastipak 50 ml syringes supplied had higher plunger forces.
It is possible that your healthcare facility's biomedical engineering service provider has already made adjustments to occlusion alarm settings to reflect these higher forces and, if so, affected syringe pumps will need to be readjusted.
The changes to plunger forces in different lots over time is illustrated in Figure 1.
It is recommended that, once new 50 ml Plastipak stock has been received, occlusion alarm settings are returned to the original levels used before May 2012. New stock is identified by a prefix "N" ahead of the product number on the case and shelf pack labels, for example "N Ref 300865".
It is important that occlusion alarm settings be reviewed to ensure that the presence of lower friction forces within the syringe do not lead to a delay in detection and annunciation of an occlusion in the fluid delivery path, leading to possible adverse patient outcomes.
Consult the syringe pump manufacturer's service documentation to determine the appropriate way to verify and adjust occlusion alarm settings for your syringe drivers.
Becton Dickinson has written to affected customers advising them of this issue.
Figure 1: Changes to pump forces for BD 50ml Plastipak syringes over time/batches
Recent safety alerts
The TGA publishes alerts on its website when there is new safety information regarding therapeutic products.
Below are TGA safety alerts relating to medical devices published since the last edition of Medical Devices Safety Update.
Medtronic Paradigm insulin pump: Health professionals are reminded of the need to advise patients to confirm insulin dosage when using certain Medtronic Paradigm insulin pump models due to the risk of over-infusion.
Medtronic SynchroMed II implantable infusion pump: Health professionals are advised that Medtronic Australasia, in consultation with the TGA, has issued a hazard alert for its SynchroMed II implantable infusion pump due to the risk of over-infusion.
Hospira infusion pumps - Plum family, GemStar and LifeCare models: Hospitals and other healthcare facilities are advised that new infusion pumps from the Plum A+ family still cannot be supplied in Australia.
Natural-Knee II System metal-backed patella: Health professionals are advised that Zimmer has issued a hazard alert regarding its Natural-Knee II System metal-backed patella due to the risk of premature implant failure.
HomeChoice PRO automated peritoneal dialysis system: Health professionals are advised that Baxter Healthcare is undertaking a recall for product correction of its HomeChoice Pro automated peritoneal dialysis system to update the Instructions for Use regarding unintended overfill.
Medtronic neurostimulation devices: Health professionals are advised that Medtronic Australasia has issued a hazard alert regarding multiple models of its neurostimulation devices due to the risk of premature battery depletion that may lead to early device replacement. Medtronic Australasia is also undertaking a recall for product correction to update the Instructions for Use.
Medtronic spinal cord stimulation devices - multiple models: Health professionals are advised that Medtronic Australasia has issued a hazard alert regarding multiple models of its spinal cord stimulation devices due to the risk of risk of spinal cord compression. Medtronic Australasia is also undertaking a recall for product correction to update the Instructions for Use.
Cereform silicone gel-filled breast implants and associated sizers: Following on from a safety advisory on 21 February regarding Cereform gel-filled breast implants, the Australian distributor has undertaken a recall of the implants and associated sizers.
FreeStyle Papillon Mini blood glucose monitoring system: Health professionals are advised that an earlier recall involving FreeStyle Lite blood glucose test strips has been extended to include FreeStyle Papillon Mini blood glucose monitors due to the potential to give potentially give incorrect blood glucose results.
 What to report? Please report adverse events, as well as near misses
What to report? Please report adverse events, as well as near misses
The TGA encourages the reporting of any suspected adverse event or potential adverse event relating to a medical device. Adverse events can involve actual harm to a patient or caregiver, or a near miss that may have resulted in harm.
Some issues relating to medical devices that may lead to adverse events and prompt you to report include:
- mechanical or material failure
- design issues
- labelling, packaging or manufacturing deficiencies
- software deficiencies
- device interactions
- user/systemic errors.
Suspected adverse events or near misses can be reported directly to the TGA:
- online at Report a problem
- by emailing iris@tga.gov.au
- by mail to IRIS, TGA, PO Box 100, Woden ACT 2606
- by fax to 02 6203 1713.
For more information about reporting, visit www.tga.gov.au or contact the TGA's Office of Product Review on 1800 809 361.
Disclaimer
The Medical Devices Safety Update (MDSU) is aimed at health professionals and is intended to provide practical information on medical device safety, including emerging safety issues. The information in the MDSU is necessarily general and is not intended to be a substitute for a health professional’s judgment in each case, taking into account the individual circumstances of their patients. Reasonable care has been taken to ensure that the information is accurate and complete at the time of publication. The Therapeutic Goods Administration gives no warranty that the information in this document is accurate or complete, and does not accept liability for any injury, loss or damage whatsoever, due to negligence or otherwise, arising from the use of or reliance on the information provided in this document.
© Commonwealth of Australia 2014
This work is copyright. You may reproduce the whole or part of this work in unaltered form for your own personal use or, if you are part of an organisation, for internal use within your organisation, but only if you or your organisation do not use the reproduction for any commercial purpose and retain this copyright notice and all disclaimer notices as part of that reproduction. Apart from rights to use as permitted by the Copyright Act 1968 or allowed by this copyright notice, all other rights are reserved and you are not allowed to reproduce the whole or any part of this work in any way (electronic or otherwise) without first being given specific written permission from the Commonwealth to do so. Requests and inquiries concerning reproduction and rights are to be sent to the TGA Copyright Officer, Therapeutic Goods Administration, PO Box 100, Woden ACT 2606 or emailed to tga.copyright@tga.gov.au.
For the latest information from the TGA, subscribe to the TGA Safety Information email list.
For correspondence or further information about Medical Devices Safety Update, contact the TGA's Office of Product Review at iris@tga.gov.au or 1800 809 361.
Medical Devices Safety Update is written by staff from the Office of Product Review.
Editor: Dr Katherine Gray
Deputy Editor: Mr Aaron Hall
TGA Principal Medical Adviser: Dr Tony Hobbs
Contributors include Dr Ying Huang, Mr Patrick O'Meley
Related content
-
Medical Devices Safety Update, Volume 2, Number 1, January 2014
Medical Devices Safety Update, Volume 2, Number 1, January 2014 -
Medical Devices Safety Update, Volume 5, Number 1, January 2017
In this issue: strategies for vena cava filter removal; ECRI lists infusion errors as top hazard; recent safety alerts -
Medical Devices Safety Update, Volume 3, Number 1, January 2015
Safety though adverse event reporting; Recommendations for avoiding or dealing with surgical implant tool breakages; IRIS inSite pilot off to promising start; Clinical alarm issues still pose top hazard; Recent safety alerts