The government is now operating in accordance with the Guidance on Caretaker Conventions, pending the outcome of the 2025 federal election.
Purpose
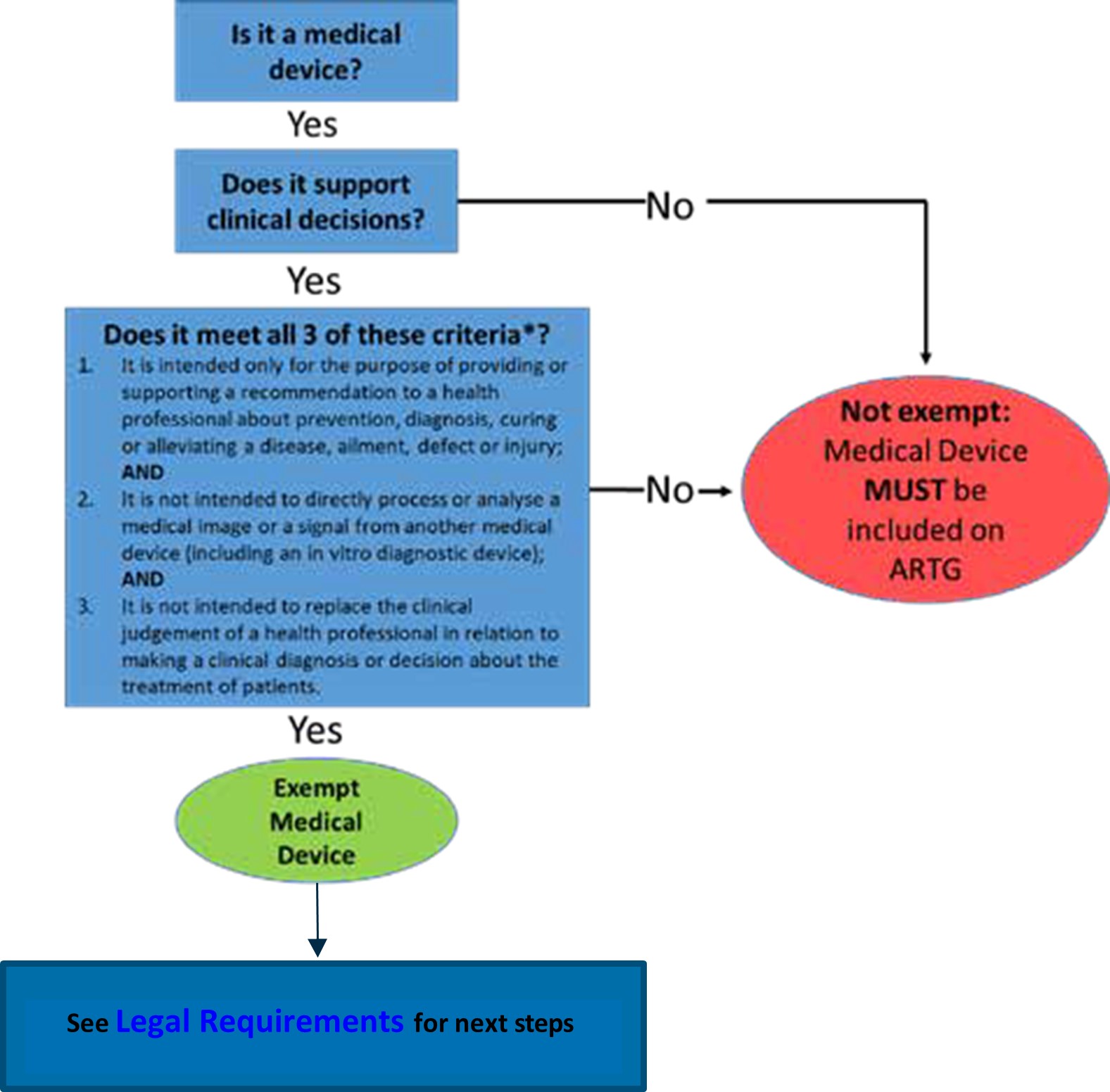
This guidance is for sponsors, manufacturers, suppliers, and software developers of Exempt Clinical Decision Support Software (CDSS) and provides detailed interpretation of the exemption criteria for certain CDSS. This is to ensure software-based medical devices meet the requirements for quality, safety, and performance. This document complements the general guidance on CDSS that was published by the TGA in February 2021.
Please note that it is the manufacturer’s responsibility to determine if a product is a medical device, according to the intended purpose of the product. Products are regulated as medical devices when they fit the definition of medical device under Section 41BD of the Therapeutic Goods Act 1989 (the Act). Sponsors, manufacturers, suppliers and software developers of CDSS products are responsible for complying with the relevant legislation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}