
We will have limited operations from 15:00 Tuesday 24 December 2024 (AEDT) until Thursday 2 January 2025. Find out how to contact us during the holiday period.
An application was submitted to include Vitamin D in Appendix H in the Poisons Standard.
This is a general application. The applicant's proposed amendments to the Poisons Standard are as follows:
Appendix H - New Entry
Vitamin D.
The applicant's reasons for the request are:
Vitamin D is currently listed in Schedule 3 and Schedule 4 of the SUSMP as follows:
Schedule 4
VITAMIN D for human internal therapeutic use except:
Schedule 3
VITAMIN D for human therapeutic use in preparations containing 175 micrograms or less of vitamin D per recommended single weekly dose except in preparations containing 25 micrograms or less of vitamin D per recommended daily dose.
Index
VITAMIN D
cross reference: COLECALCIFEROL, ERGOCALCIFEROL
Schedule 4
Schedule 3
In October 2012, the ACMS considered a proposal by the same applicant to create a new Schedule 3 entry for vitamin D to allow a weekly dose up to 175 micrograms per recommended dose and to include vitamin D in Appendix H. The ACMS supported the proposal to allow the higher weekly dose, but advised against an Appendix H entry. Some members supported the Appendix H entry, stating that it would promote awareness of the weekly dosage regime. Other members did not support the Appendix H entry as public health activities were considered sufficient to promote appropriate use of vitamin D. There were also concerns about off label use and no limits on pack sizes. The committee also noted that other vitamin D products, as different formulations, were unscheduled and could be advertised. The delegate made a final decision (8 February 2013) to include vitamin D, as a single weekly dose of up to 175 micrograms (7000 IU), in Schedule 3 and not to include vitamin D in Appendix H.
Vitamin D is available primarily as colecalciferol (vitamin D3, Figure 3.1A), and ergocalciferol (vitamin D2, Figure 3.1 B).
The major natural source of vitamin D in humans comes from the action of ultraviolet light on 7 dehydrocholesterol in the skin to form provitamin D3 which is then converted to colecalciferol.
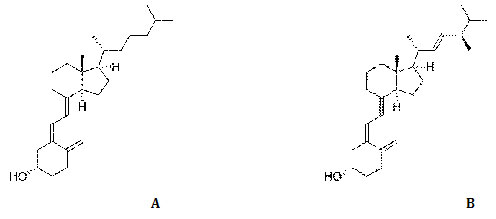
Figure 3.1: Structures of colecalciferol (A) and ergocalciferol (B)
| Property |
| Ergocalciferol (vitamin D2) |
|---|---|---|
| INN/BAN/AAN | colecalciferol | ergocalciferol |
| CAS No. | 67-97-0 | 50-14-6 |
| Chemical name | (5Z,7E)-9,10-secocholesta-5,7,10(19)-trien-3β-ol | (5Z,7E,22E)-9,10-secoergosta-5,7,10(19),22-tetraen-3β-ol |
| Molecular formula | C27H44O | C28H44O |
| Units | 25 micrograms = 1000 IU 175 micrograms = 7000 IU | - |
| Molecular Weight | 384.6 | 396.7 |
Four (4) public submissions were received and all supported the proposal. The main points were:
The committee advised that Vitamin D be entered in Appendix H of the Poisons Standard.
The committee also recommended an implementation date of 1 June 2017.
The matters under subsection 52E (1) of the Therapeutic Goods Act 1989 considered relevant by the committee included: a) the risks and benefits of the use of a substance; b) the purposes for which a substance is to be used and the extent of use of a substance; c) the toxicity of a substance; d) the dosage, formulation, labelling, packaging and presentation of a substance; e) the potential for abuse of a substance; f) any other matters that the Secretary considers necessary to protect the public health.
The reasons for the advice comprised the following:
The delegate considered the following in regards to this proposal:
The delegate's interim decision is to create a new Appendix H entry for Vitamin D.
The current Schedule 3 entry for vitamin D and proposed Appendix H entry are as follows:
Schedule 3 - Current entry
VITAMIN D for human therapeutic use in preparations containing 175 micrograms or less of vitamin D per recommended single weekly dose except in preparations containing 25 micrograms or less of vitamin D per recommended daily dose.
Appendix H - New Entry
VITAMIN D
The proposed implementation date is 1 June 2017.
The matters under subsection 52E (1) of the Therapeutic Goods Act 1989 considered relevant by the delegate included: a) the risks and benefits of the use of the substance; b) the purposes for which a substance is to be used and the extent of use of a substance; c) the toxicity of the substance; d) the dosage, formulation, labelling, packaging and presentation of a substance; e) the potential for abuse of a substance; and f) any other matters that the Secretary considers necessary to protect public health.
The reasons for the recommendation comprised the following: